|
Replies: 16
| visibility 1
|
All-TigerNet [12592]
TigerPulse: 100%
Posts: 6312
Joined: 12/24/15
|
COVID is a disease of the unvaccinated ?
Jun 15, 2022, 3:03 PM
|
|
Fauci who has had 2 shots plus 2 boosters has COVID. Did he not care enough about others to double mask?
Fortunately he’s experiencing mild symptoms probably due to his quad vax status, but firing folks who refused the shot look very punitive at this point.
|
|
|
|
 |
All-TigerNet [12161]
TigerPulse: 100%
Posts: 17894
Joined: 5/16/00
|
Severe COVID is a disease of the unvaccinated
Jun 15, 2022, 3:12 PM
|
|
fixed it for you
|
|
|
|
|
|
All-In [47795]
TigerPulse: 100%
Posts: 44515
Joined: 9/5/02
|
rons1 be like
Jun 15, 2022, 3:14 PM
|
|

|
|
|
|
|
|
All-TigerNet [12592]
TigerPulse: 100%
Posts: 6312
Joined: 12/24/15
|
Re: rons1 be like
Jun 15, 2022, 3:51 PM
|
|
You just shidd yourself with that attempt at playing the pigeon hole game.
|
|
|
|
|
|
All-TigerNet [12592]
TigerPulse: 100%
Posts: 6312
Joined: 12/24/15
|
Re: Severe COVID is a disease of the unvaccinated
Jun 15, 2022, 3:38 PM
[ in reply to Severe COVID is a disease of the unvaccinated ] |
|
fixed it for you
fixed it for you
True. I said as much. I took both shots. I’ve taken one booster. I’m holding off on another booster until such booster offers more protection than the original shot.
My point is that a lot of folks were demonized for not taking the shot which we now know does not prevent infection nor spread of the disease.
We were led to believe that if only everyone took the vaccine we could “shut down” the virus.
Maybe we could’ve had a chance with that had we been able to quickly vaccinate the entire world early on.
Nuance guys. I’m not anti vaccine, but much of what we were told just wasn’t ultimately true.
|
|
|
|
|
|
All-TigerNet [12161]
TigerPulse: 100%
Posts: 17894
Joined: 5/16/00
|
gotcha, and yes and no
Jun 15, 2022, 3:53 PM
|
|
studies I've read show that there is less transmission in higher % vaccinated populations. Studies won't ever really be that good because they aren't controlled, just retrospective, but is what it is
Makes sense, less sick you are, less viral load, less transmission
Every vaccine has some non responders and breakthrough infections, just covid was higher
|
|
|
|
|
|
All-TigerNet [12592]
TigerPulse: 100%
Posts: 6312
Joined: 12/24/15
|
Re: gotcha, and yes and no
Jun 15, 2022, 3:55 PM
|
|
Agree.
|
|
|
|
|
|
All-In [40929]
TigerPulse: 100%
Posts: 42947
Joined: 11/30/98
|
Back when it was 90% effective
Jun 15, 2022, 4:00 PM
[ in reply to gotcha, and yes and no ] |
|
6 people in my office all on the same day, which is 100% of the people that were in my office that day got covid. 1 client and 5 coworkers. I knew they were full of #### for sure that day. They had to have similar data. They started coming clean about that time too and started to admit that the vaccine did not prevent transmission.
Supposedly it was 90% effective. 6 out of 6 people at 90% effective would be a (.1)^6 chance that all got it or 1 in 1 million chance.
It had to take its course. All the fear mongering in the world was not going to change a thing.
|
|
|
|
|
|
All-TigerNet [12161]
TigerPulse: 100%
Posts: 17894
Joined: 5/16/00
|
|
|
|
|
|
All-In [40929]
TigerPulse: 100%
Posts: 42947
Joined: 11/30/98
|
that's my point
Jun 15, 2022, 5:11 PM
|
|
they are clearly full of ####
|
|
|
|
|
|
Oculus Spirit [97716]
TigerPulse: 100%
Posts: 64855
Joined: 7/13/02
|
Since NBC omitted the study
Jun 21, 2022, 12:14 PM
|
|
here it is.
https://www.medrxiv.org/content/10.1101/2021.09.28.21264260v2.full-text The impact of SARS-CoV-2 vaccination on Alpha & Delta variant transmission Background Pre-Delta, vaccination reduced SARS-CoV-2 transmission from individuals infected despite vaccination, potentially via reducing viral loads. While vaccination still lowers the risk of infection, similar viral loads in vaccinated and unvaccinated individuals infected with Delta question how much vaccination prevents transmission. Methods We performed a retrospective observational cohort study of adult contacts of SARS-CoV-2-infected adult index cases using English contact testing data. We used multivariable Poisson regression to investigate associations between transmission and index case and contact vaccination, and how these vary with Alpha and Delta variants (classified using S-gene detection/calendar trends) and time since second vaccination. Results 54,667/146,243(37.4%) PCR-tested contacts of 108,498 index cases were PCR-positive. Two doses of BNT162b2 or ChAdOx1 vaccines in Alpha index cases were independently associated with reduced PCR-positivity in contacts (aRR, adjusted rate ratio vs. unvaccinated=0.32[95%CI 0.21-0.48] and 0.48[0.30-0.78] respectively). The Delta variant attenuated vaccine-associated reductions in transmission: two BNT162b2 doses reduced Delta transmission (aRR=0.50[0.39-0.65]), more than ChAdOx1 (aRR=0.76[0.70-0.82]). Variation in Ct values (indicative of viral load) explained 7-23% of vaccine-associated transmission reductions. Transmission reductions declined over time post-second vaccination, for Delta reaching similar levels to unvaccinated individuals by 12 weeks for ChAdOx1 and attenuating substantially for BNT162b2. Protection in contacts also declined in the 3 months post-second vaccination. Conclusions Vaccination reduces transmission of Delta, but by less than the Alpha variant. The impact of vaccination decreased over time. Factors other than PCR Ct values at diagnosis are important in understanding vaccine-associated transmission reductions. Booster vaccinations may help control transmission together with preventing infections. ### Competing Interest Statement DWE declares lecture fees from Gilead outside the submitted work. No other author has a conflict of interest to declare. ### Funding Statement This study was funded by the UK Government's Department of Health and Social Care. This work was supported by the National Institute for Health Research Health Protection Research Unit (NIHR HPRU) in Healthcare Associated Infections and Antimicrobial Resistance at Oxford University in partnership with Public Health England (PHE) (NIHR200915), and the NIHR Biomedical Research Centre, Oxford. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health or Public Health England. DWE is a Robertson Foundation Fellow and an NIHR Oxford BRC Senior Fellow. ASW is an NIHR Senior Investigator. ### Author Declarations I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained. Yes The details of the IRB/oversight body that provided approval or exemption for the research described are given below: The study was performed as public health surveillance and NHS Test and Trace program quality assurance, under Section 251 of the NHS Act 2006 with approvals from Public Health England (PHE), the Department of Health and Social Care and NHS Test and Trace. PHE's Research Ethics and Governance Group (PHE's Research Ethics Committee) reviewed the study protocol and confirmed compliance with all regulatory requirements. As no regulatory or ethical issues were identified, it was agreed that full ethical review was not needed, and the protocol was approved. I confirm that all necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived, and that any patient/participant/sample identifiers included were not known to anyone (e.g., hospital staff, patients or participants themselves) outside the research group so cannot be used to identify individuals. Yes I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance). Yes I have followed all appropriate research reporting guidelines and uploaded the relevant EQUATOR Network research reporting checklist(s) and other pertinent material as supplementary files, if applicable. Yes Applications to use the data in this study can be made to NHS Digital's Data Access Request Service, please see <url=https://www.medrxiv.org/content/10.1101/0.32[95%CI 0.21-0.48] and 0.48[0.30-0.78] respectively). The Delta variant attenuated vaccine-associated reductions in transmission: two BNT162b2 doses reduced Delta transmission (aRR=0.50[0.39-0.65]), more than ChAdOx1 (aRR=0.76[0.70-0.82]). Variation in Ct values (indicative of viral load) explained 7-23% of vaccine-associated transmission reductions. Transmission reductions declined over time post-second vaccination, for Delta reaching similar levels to unvaccinated individuals by 12 weeks for ChAdOx1 and attenuating substantially for BNT162b2. Protection in contacts also declined in the 3 months post-second vaccination. Conclusions Vaccination reduces transmission of Delta, but by less than the Alpha variant. The impact of vaccination decreased over time. Factors other than PCR Ct values at diagnosis are important in understanding vaccine-associated transmission reductions. Booster vaccinations may help control transmission together with preventing infections. ### Competing Interest Statement DWE declares lecture fees from Gilead outside the submitted work. No other author has a conflict of interest to declare. ### Funding Statement This study was funded by the UK Government's Department of Health and Social Care. This work was supported by the National Institute for Health Research Health Protection Research Unit (NIHR HPRU) in Healthcare Associated Infections and Antimicrobial Resistance at Oxford University in partnership with Public Health England (PHE) (NIHR200915), and the NIHR Biomedical Research Centre, Oxford. The views expressed in this publication are those of the authors and not necessarily those of the NHS, the National Institute for Health Research, the Department of Health or Public Health England. DWE is a Robertson Foundation Fellow and an NIHR Oxford BRC Senior Fellow. ASW is an NIHR Senior Investigator. ### Author Declarations I confirm all relevant ethical guidelines have been followed, and any necessary IRB and/or ethics committee approvals have been obtained. Yes The details of the IRB/oversight body that provided approval or exemption for the research described are given below: The study was performed as public health surveillance and NHS Test and Trace program quality assurance, under Section 251 of the NHS Act 2006 with approvals from Public Health England (PHE), the Department of Health and Social Care and NHS Test and Trace. PHE's Research Ethics and Governance Group (PHE's Research Ethics Committee) reviewed the study protocol and confirmed compliance with all regulatory requirements. As no regulatory or ethical issues were identified, it was agreed that full ethical review was not needed, and the protocol was approved. I confirm that all necessary patient/participant consent has been obtained and the appropriate institutional forms have been archived, and that any patient/participant/sample identifiers included were not known to anyone (e.g., hospital staff, patients or participants themselves) outside the research group so cannot be used to identify individuals. Yes I understand that all clinical trials and any other prospective interventional studies must be registered with an ICMJE-approved registry, such as ClinicalTrials.gov. I confirm that any such study reported in the manuscript has been registered and the trial registration ID is provided (note: if posting a prospective study registered retrospectively, please provide a statement in the trial ID field explaining why the study was not registered in advance). Yes I have followed all appropriate research reporting guidelines and uploaded the relevant EQUATOR Network research reporting checklist(s) and other pertinent material as supplementary files, if applicable. Yes Applications to use the data in this study can be made to NHS Digital's Data Access Request Service, please see < https://digital.nhs.uk/services/data-access-request-service-dars> for more details.
|
|
|
|
|
|
All-In [40929]
TigerPulse: 100%
Posts: 42947
Joined: 11/30/98
|
|
|
|
|
|
All-TigerNet [12161]
TigerPulse: 100%
Posts: 17894
Joined: 5/16/00
|
yeah that was about as accurate
Jun 15, 2022, 4:28 PM
|
|
as preseason football polls
|
|
|
|
|
|
Oculus Spirit [97716]
TigerPulse: 100%
Posts: 64855
Joined: 7/13/02
|
|
|
|
|
|
Hall of Famer [21576]
TigerPulse: 100%
Posts: 13918
Joined: 9/7/02
|
Agree.
Jun 15, 2022, 3:24 PM
|
|
It should be their choice if they want to risk death and/or cause it to mutate to something worse.
|
|
|
|
|
|
Oculus Spirit [97716]
TigerPulse: 100%
Posts: 64855
Joined: 7/13/02
|
Wait, the slash separated troof from fiction
Jun 15, 2022, 4:24 PM
|
|
Vaccines help you not die. Natural immunity helps you not die (but with a greater chance of dying getting immunity). That's it. Nothing prevents, or stops transmission. We literally lack the biology to stop transmission of viruses that inhibit MHC1 expression. That's colds, flu, HIV, and many other viruses. We can't stop those viruses. There is no such thing as "natural" immunity with those viruses, to stop them. Covid is on that list. "Immunity" with covid is only how well you clear the virus once infected.
The flow chart starts with an infected cell releasing MHC1 markers. Step two you have interferons that pick up on the MHC1 markers and call in T cells. T cells identify the virus call in the best antibodies to kill the virus. Covid short circuits our immunity literally AT STEP #1, before step 1 really.
Then there's a backend process after infection where your immune system is damaged. T cells are attacked and killed by even mild covid infections. So when you recover, you're overall going to have a weaker (normal) immune response to the next infection, which occurs in about 7 months on average. While all this is going on, the virus is mutating, and the new variants end up having to "vary" less and less to reinfect you, as your immune system is weaker. Then you're exposed to a variant, MHC1 is blocked, and you get infected again, with less T cells to respond, with antibodies that are not perfect as it has mutated, and then you get sick again, recover, but with a few less T cells. Repeat process.
We knew MHC1 was blocked by covid in May of 2020, thanks to China. Study below is why vaccines and natural immunity don't work. Shown LONG before vaccines. I didn't trust Fauci long before covid anyway. Goes back to H1N1 in 2009.
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7189399/
This decreases interferon response, also seen in 2020. Again all this is before the mighty T cells come into play. You know, the cells we were told would save us and end the pandemic and give us "herd immunity".
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7249038/
And then you have post covid T cell apoptosis, which causes lower killer T cells, and white cell counts in covid patients. This, BTW, opens people up to more OTHER viruses and infections, causing rare viruses we normally handle, to cause many more illnesses due to weakened immune systems. Plus, common viruses present as more severe, or with different symptoms.
https://onlinelibrary.wiley.com/doi/10.1002/jmv.26742
And finally, you have Omicron attacking T cells directly, and it's attaching to them and killing them using different cell attachment and entry mechanisms, not ACE 2 like it uses in normal cells.
https://www.nature.com/articles/s41392-022-00919-x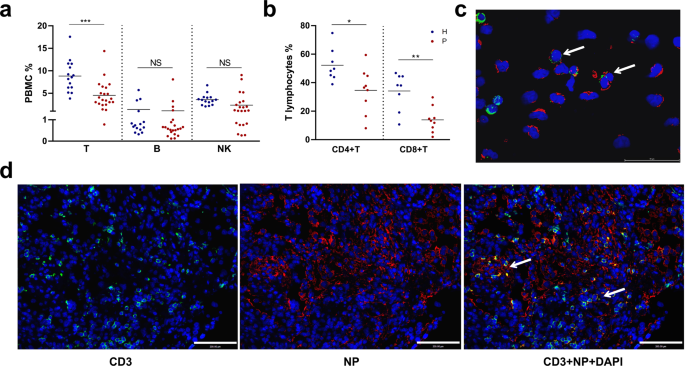 ACE2-independent infection of T lymphocytes by SARS-CoV-2 - Signal Transduction and Targeted Therapy SARS-CoV-2 induced marked lymphopenia in severe patients with COVID-19. However, whether lymphocytes are targets of viral infection is yet to be determined, although SARS-CoV-2 RNA or antigen has been identified in T cells from patients. Here, we confirmed that SARS-CoV-2 viral antigen could be detected in patient peripheral blood cells (PBCs) or postmortem lung T cells, and the infectious virus could also be detected from viral antigen-positive PBCs. We next prove that SARS-CoV-2 infects T lymphocytes, preferably activated CD4 + T cells in vitro. Upon infection, viral RNA, subgenomic RNA, viral protein or viral particle can be detected in the T cells. Furthermore, we show that the infection is spike-ACE2/TMPRSS2-independent through using ACE2 knockdown or receptor blocking experiments. Next, we demonstrate that viral antigen-positive T cells from patient undergone pronounced apoptosis. In vitro infection of T cells induced cell death that is likely in mitochondria ROS-HIF-1a-dependent pathways. Finally, we demonstrated that LFA-1, the protein exclusively expresses in multiple leukocytes, is more likely the entry molecule that mediated SARS-CoV-2 infection in T cells, compared to a list of other known receptors. Collectively, this work confirmed a SARS-CoV-2 infection of T cells, in a spike-ACE2-independent manner, which shed novel insights into the underlying mechanisms of SARS-CoV-2-induced lymphopenia in COVID-19 patients.
So in summary, Fauci is full of crap. Has been since day 1, before day one, was last decade. Covid won't go away because of what it does on both the front end of infection, and what it leaves you with after you recover. There are many other impacts, but these are the most important ones to know. Over time we will die less from it, but the living with it part is what will be toughest. There will be many mysteries we just don't understand. Like mysterious inflation, mysterious labor shortages, mysterious hepatitis in kids, mysterious monkeypox, mysterious fungal infections,....it will be a long and growing list.
But that's the role of the Fauci's of the world, and the Biden's and the Trump's of the world. As long as we can blame them for everything, all is well. And if they won't accept responsibility, there's always Putin.
|
|
|
|
|
|
Orange Blooded [4679]
TigerPulse: 100%
Posts: 6557
Joined: 4/11/20
|
Re: COVID is a disease of the unvaccinated ?
Jun 15, 2022, 4:51 PM
|
|
Well I had Covid 19 months ago and I remain unvaccinated so I guess it’s a disease of the unvaccinated. Well, except for every single vaccinated person I know who has also had Covid. Got it.
|
|
|
|
|
|
Replies: 16
| visibility 1
|
|
|











{kind=link}